 +91- 9692108108
+91- 9692108108
Traumatic Spine Fracture & Emergency Stabilization
(24/7 spine trauma care, rapid stabilization, and emergency spine surgery by Dr Abhishek Mannem | Bangalore Back)
Traumatic spine injuries arrive without warning. A late‑night two‑wheeler crash on NICE Road, a fall from a scaffolding site in Peenya, or a gym mishap that didn’t look serious at first—these are the real stories I see in our emergency room. In these moments, the first question I ask myself is simple: is the spinal cord safe? Because bones can be fixed; the spinal cord does not forgive delays. At Bangalore Back, our pathway prioritises rapid imaging, immediate stabilization, and early surgical planning. This tight, time‑bound approach prevents the silent enemy in trauma—secondary injury.
Understanding Traumatic Spine Fractures
A spinal fracture is not just a broken vertebra. Trauma can shift alignment, tear stabilising ligaments, or push bone fragments into the spinal canal. Some patients are able to walk into the hospital, yet carry a hidden instability that worsens with a small twist or an attempt to sit. The most common reason for deterioration before reaching us is incorrect handling—lifting, turning or transporting without spinal immobilisation. The single best rule until imaging is done: keep the spine neutral and avoid unnecessary movement.
Types of Traumatic Spine Fractures
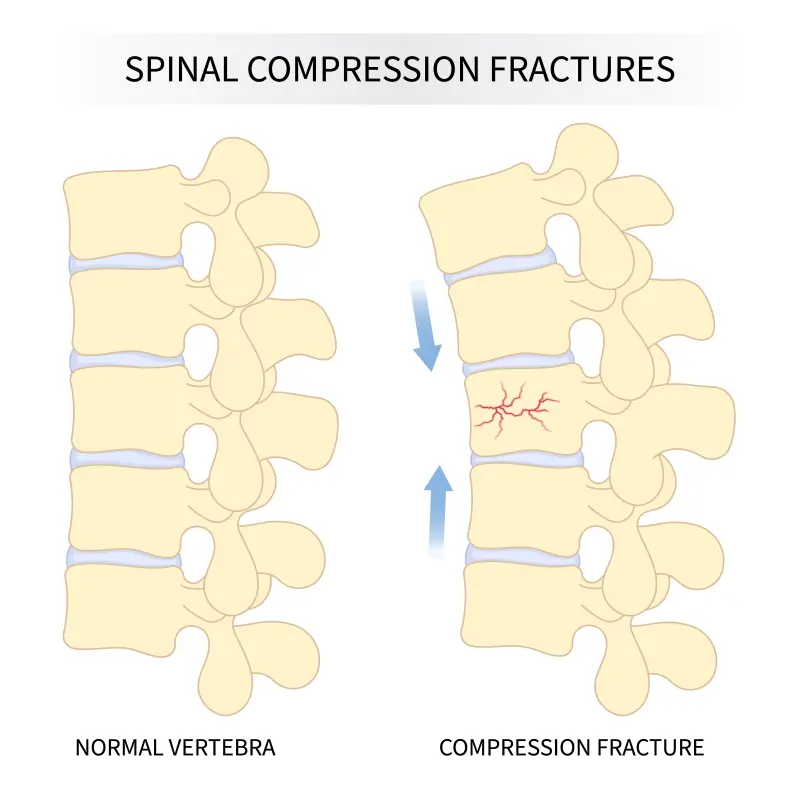
- Compression fractures – partial collapse after axial load or sudden impact
- Burst fractures – vertebral body shatters; fragments may narrow the spinal canal
- Flexion‑distraction (Chance) injuries – often seat‑belt related in high‑velocity crashes
- Fracture‑dislocations – severely unstable, frequently causing neurological deficits
- Cervical fractures (C1–C7) – high risk due to proximity to breathing pathways
- Rotational / translational injuries – vertebra twists or shifts out of alignment
Common Causes
- Two‑wheeler accidents on urban expressways and highways across Bengaluru & South India
- Falls from height at construction/industrial sites (Peenya, Bidadi, Electronic City)
- Sports and gym injuries with sudden, uncontrolled impact
- Industrial heavy‑object trauma and machinery accidents
- Osteoporotic collapse aggravated by a minor fall in older adults
Symptoms and Warning Signs
- Sudden severe neck or back pain after trauma
- Tingling, numbness, or ‘electric shock’ sensations into arms or legs
- Weakness, foot‑drop, imbalance, or frequent collapsing
- Loss of bladder or bowel control (treat as an emergency)
- Visible deformity, painful spasm, or inability to stand
- Feeling that the spine is ‘giving way’ with movement
Many of my elderly patients benefit from these techniques because the recovery is smoother and muscle pain is minimal.
Emergency Management at Bangalore Back
Our trauma response begins the moment a spine injury is suspected:
- Spinal immobilisation during ambulance transport
- ABC stabilisation in the ER; haemodynamic support
- Whole‑spine CT for fracture mapping
- MRI for cord compression, oedema and ligamentous injury
- ASIA neurological grading to document baseline function
- Early decision making—external bracing vs. urgent surgical stabilisation
- Neuro‑ICU when polytrauma or respiratory risk is present
When Surgery Is Required
Surgery is advised when there is neurological weakness, cord compression on MRI, high‑grade instability (AO Type B/C), burst fracture with canal compromise, fracture‑dislocation, traumatic spondylolisthesis, or progressive symptoms. In unstable trauma, waiting is often more dangerous than operating.
Surgical Techniques at Bangalore Back
Every fracture pattern is different; the plan is individualised:
- Navigation‑guided pedicle screw fixation for high accuracy
- Posterior long‑segment instrumentation for extensive instability
- Anterior corpectomy with cage reconstruction when canal is compromised
- Minimally invasive stabilisation to preserve muscle envelope (selected cases)
- Decompression to clear bone fragments / haematoma impinging the cord or roots
 Request an appointment
Request an appointment
Lorem ipsum dolor

Why Patients Choose Bangalore Back
- 24/7 emergency spine team with dedicated trauma pathways
- Rapid access to CT, MRI, trauma OT and Neuro‑ICU under one roof
- Navigation and robotics for precision in complex or multi‑level fractures
- Personal involvement by Dr Abhishek Mannem through surgery and rehabilitation
- Strong outcomes in delayed referrals and complex, multi‑system trauma
Before & After Clinical Gallery
We showcase real patient cases (with consent), including:
- Pre- and Post-operative MRIs and X-rays
- Disc Herniations, Stenosis, and Spondylolisthesis cases
- Visible improvement in alignment and decompression


Recovery And Rehabilitation

Rehabilitation starts early once the spine is secure. We aim for:
- Mobilisation within 48–72 hours when safe
- Bracing for cervical or thoraco‑lumbar injuries when indicated
- Respiratory training in high cervical trauma
- Progressive strengthening, balance and gait re‑training
- Bladder–bowel rehab and occupational therapy for neurological injuries
- Education on posture, safe lifting, and long‑term spine health
FAQ’s
Is every spine fracture an emergency?
How soon should surgery be done?
Can paralysis be reversed?
Do implants remain permanently?
How long is the hospital stay?

Let’s Start Fixing Your Back, Together.
Whether it’s a nagging pain, an unclear diagnosis, or a question about surgery—your spine deserves expert attention. Schedule a one-on-one consultation with Dr. Abhishek Mannem and get a personalized path to recovery.